By Hilary Gerber and Amy Romano
This article is part of A Woman's Guide to VBAC: Navigating the NIH Consensus Recommendations, a collection of resources that address the most common and pressing questions women may have about their birth choices. View all sections in the guide, including a link to the authors, on the index page.
Vaginal births after prior cesareans (VBAC s) were not always as uncommon as they are now. The frequency of attempted VBACs in the United States in recent decades has been associated with reactions to statements published by two major medical organizations: the American Congress of Obstetricians and Gynecologists (ACOG), and the National Institutes of Health (NIH). The most significant impact on VBAC access came with ACOG's so-called "immediately available" standard.
What Is the "Immediately Available" Standard and What Was its Immediate Effect?
In 1999, three years after a widely publicized but also widely criticized study was published (MacMahon et al., 1996), ACOG changed their practice bulletin on VBAC to include the recommendation that " VBAC should be attempted in institutions equipped to respond to emergencies with physicians immediately available to provide emergency care." (ACOG, 1999) This practice bulletin also recommended that a physician "capable of monitoring labor and performing an emergency cesarean delivery" be "immediately available throughout active labor," and that anesthesia and personnel for an emergency cesarean be "available." The "[i]nability to perform emergency cesarean delivery because of unavailable surgeon, anesthesia, sufficient staff or facility" was considered to be a contraindication for VBAC.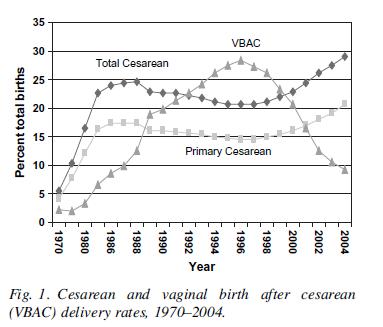
These recommendations were given a Level C rating, which means they were based on consensus and expert opinion, not research. The recommendation that "most women" who were good candidates for VBACs "should be counseled about VBAC and offered a trial of labor," on the other hand, was a Level A recommendation, which means it is "based on good and consistent scientific evidence."
Unfortunately, the lower rated recommendation for immediately available emergency surgery was interpreted by many institutions to mean 24 hour in-house obstetrics and anesthesia must be present to allow a trial of labor after cesarean, and has prevented the higher rated recommendation to offer VBAC to eligible patients from being actualized.(Guise J-M et al., 2010) This has led to serious barriers to planned VBAC for women who are good candidates and desire a chance at vaginal birth.
This "immediately available" standard was not explained in any more detail in ACOG's practice bulletin on vaginal delivery after cesarean, but it was expanded on in a later ACOG committee opinion on anesthesia and obstetrics as "a local decision based on each institution's available resources and geographic location." (American College of Obstetricians and Gynecologists and American Society of Anesthesiologists, 2009) Even though this explanation clearly allows for a very flexible definition of "immediately available" that takes into account individual hospital characteristics, the reaction of many smaller, more geographically remote hospitals was to ban VBACs if they could not provide in-house anesthesia and continuous supervision by an ob/gyn. One study of hospitals in a large geographic region noted that more than 30% of institutions that previously offered VBAC before the change in the guidelines were no longer allowing them.(Roberts et al., 2007) In a 2006 survey of women who gave birth in U.S. hospitals, 57% of mothers who had a prior cesarean and wanted to try for a VBAC were refused the chance, and 68% reported it was due to the unwillingness of their provider or hospital, and only 20% said there was a medical reason given. (Declercq et al., 2006)
What Did the NIH Consensus Panel Recommend Regarding the Immediately Available Standard?
When the NIH Consensus Panel looked at the "immediately available" standard, the evidence was mixed when discussing the relationship between "decision to incision", or time between signs that a cesarean section may be necessary (in the case of uterine rupture, that would usually be fetal heart rate decelerations) and performing the cesarean section. Two large studies that examine how that response time may influence poor fetal outcomes were included in this evidence report. All of the research was done in hospitals with in-house anesthesia and obstetrics, and there were still occasional fetal deaths, and no consistent evidence that a quicker response or in house anesthesia made could prevent the extremely rare fetal death. The NIH Consensus Panel concluded that the evidence on response time was "insufficient", but they did suggest that fetal bradycardia, or slow heart rate, should indicate a "prompt delivery". No studies compared in-house obstetrics and anesthesia to on call obstetrics and anesthesia.
In addition, Anne Lyerly, a prominent obstetrician and bioethicist who has written as a member of the Obstetrics and Gynecology Risk Group in ACOG's journal Obstetrics and Gynecology, testified at the 2010 NIH VBAC Consensus Development Conference. She argued that the absolute risk for fetal death for both VBAC attempts and a first time (also known as primary) vaginal delivery are practically identical. (See Putting Uterine Rupture into Perspective in this Guide). She warns that distorting risk and limiting informed choice in this manner "can lead to care that is neither evidence-based nor patient-centered, often to the detriment of both women and infants." (Lyerly et al., 2007)
ACOG's Response and New Guidelines
In the wake of the NIH Consensus Conference, the Editor-in-Chief of Obstetrics & Gynecology, ACOG's peer-reviewed journal, devoted his editorial to calling for reconsideration of the immediate availability standard. Consumer advocates also waged a campaign to convince ACOG to revisit the standard. And indeed, in July 2010, ACOG released an updated version of their practice bulletin on VBAC (American Congress of Obstetrics and Gynecologists, 2010). Although the bulletin still recommends that VBACs occur in facilities capable of providing immediately available emergency care, the following caveats were added to this recommendation:
When resources for immediate cesarean delivery are not available, the College recommends that health care providers and patients considering [trial of labor after cesarean] discuss the hospital's resources and availability of obstetric, pediatric, anesthetic, and operating room staffs. Respect for patient autonomy supports that patients should be allowed to accept increased levels of risk, however, patients should be clearly informed of such potential increase in risk and management alternatives.
Although it is still too early to tell whether or not these new guidelines have made any significant changes in VBAC availability throughout the United States, the changes themselves are significant in their own right. To clarify, women can now challenge hospitals and/or care providers who have instituted VBAC bans by referring to ACOG's own claims about respect for patient autonomy and responsibility. For it is a woman's responsibility to be apprised of the potential increase in risk, but it is also her right to take on such risks as she sees fit.
Despite these very important changes, women will still face hospitals and providers that refuse to "offer" VBAC because of inability to intervene "immediately" should an urgent complication develop in a VBAC labor. Other sections of this guide offer suggestions for putting the risks of VBAC into perspective and taking action at the community level to improve access to VBAC.
Additional Reading
References
1. American College of Obstetricians and Gynecologists and American Society of Anesthesiologists (2009). ACOG committee opinion No. 433: optimal goals for anesthesia care in obstetrics. Obstet.Gynecol., 113, 1197-1199.
2. American College of Obstetricians and Gynecologists (1999). Practice Bulletin #5. "Vaginal Birth after Previous Cesarean Section"
3. American Congress of Obstetricians and Gynecologists (2010). Practice Bulletin #115. "Vaginal Birth after Previous Cesarean Delivery."
4. Declercq, E., Sakala, C., Corry, M. P., & Applebaum, S. (2006). Listening to Mothers II: Report of the Second National Survey of Women's Childbearing Experiences New York: Childbirth Connection.
5. Guise J-M, Eden K, Emeis C, Denman MA, Marshall N, Fu R et al. (2010). Vaginal Birth After Cesarean: New Insights (Rep. No. 191). Rockville, MD: Agency for Healthcare Research and Quality.
6. Lyerly, A. D., Mitchell, L. M., Armstrong, E. M., Harris, L. H., Kukla, R., Kuppermann, M. et al. (2007). Risks, values, and decision making surrounding pregnancy. Obstet.Gynecol., 109, 979-984.
7. McMahon, M. J., Luther, E. R., Bowes, W. A., Jr., & Olshan, A. F. (1996). Comparison of a trial of labor with an elective second cesarean section. N.Engl.J.Med., 335, 689-695.
8. Roberts, R. G., Deutchman, M., King, V. J., Fryer, G. E., & Miyoshi, T. J. (2007). Changing policies on vaginal birth after cesarean: impact on access. Birth, 34, 316-322.
Tags
Birth Preparing for VBAC A Woman's Guide to VBAC